All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit the International Myeloma Foundation or HealthTree for Multiple Myeloma.
The Multiple Myeloma Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the Multiple Myeloma Hub cannot guarantee the accuracy of translated content. The Multiple Myeloma Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The Multiple Myeloma Hub is an independent medical education platform, sponsored by Bristol Myers Squibb, GSK, Johnson & Johnson Innovative Medicine, Legend Biotech, Pfizer, Roche, and Caribou Biosciences. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account to access:
Bookmark & personalize site content
Receive alerts for new content in your areas of interest
View multiple myeloma content recommended for you
Talquetamab in R/R MM: Updates from the MonumenTAL trials
G protein-coupled receptor family C group 5 member D (GPRC5D) is a promising immunotherapy target for patients with multiple myeloma (MM) due to its high expression on malignant plasma cells.1 Talquetamab is an investigational bispecific T-cell engager antibody targeting both the GPRC5D and CD3 molecules for the treatment of patients with relapsed/refractory (R/R) MM.1 As a result of encouraging phase I and II trial results, a biologics license application for the bispecific antibody talquetamab was submitted to the U.S. Food and Drug Administration (FDA) on December 9, 2022.
Recently, the final analysis results of the phase I MonumenTAL-1 trial investigating the dose escalation of talquetamab were published in the New England Journal of Medicine by Ajai Chari et al.1 This was shortly followed by a presentation of the combined phase I and II results at the 64th American Society of Hematology (ASH) Annual Meeting and Exposition by Chari.2 Prospective phase III trials were also presented at the congress. Below, we summarize results from the phase I and II parts of the MonumenTAL-1 trial, as well as outline future phase III studies.
MonumenTAL-1: Final phase I results1
The Multiple Myeloma Hub previously reported the study protocol and patient characteristics from the phase I trial. MonumenTAL-1 is an ongoing phase I/II study of talquetamab in patients with R/R MM (NCT03399799). The key objective is to evaluate the efficacy and safety of the recommended phase II dose.
Overall, 232 patients with no prior exposure to T-cell redirecting therapies received talquetamab intravenously (n = 102) and subcutaneously (n = 130). The final response rates from talquetamab are shown in Figure 1. The median time to response and median duration of response for patients treated with 0.4 mg/kg was 0.9 months and 10.2 months, respectively. In contrast, the median time to response and median duration of response for patients treated with 0.8 mg/kg was 1.2 months and 7.8 months, respectively.
Figure 1. Best response rates for patients treated with 0.4 mg/kg and 0.8 mg/kg of talquetamab*
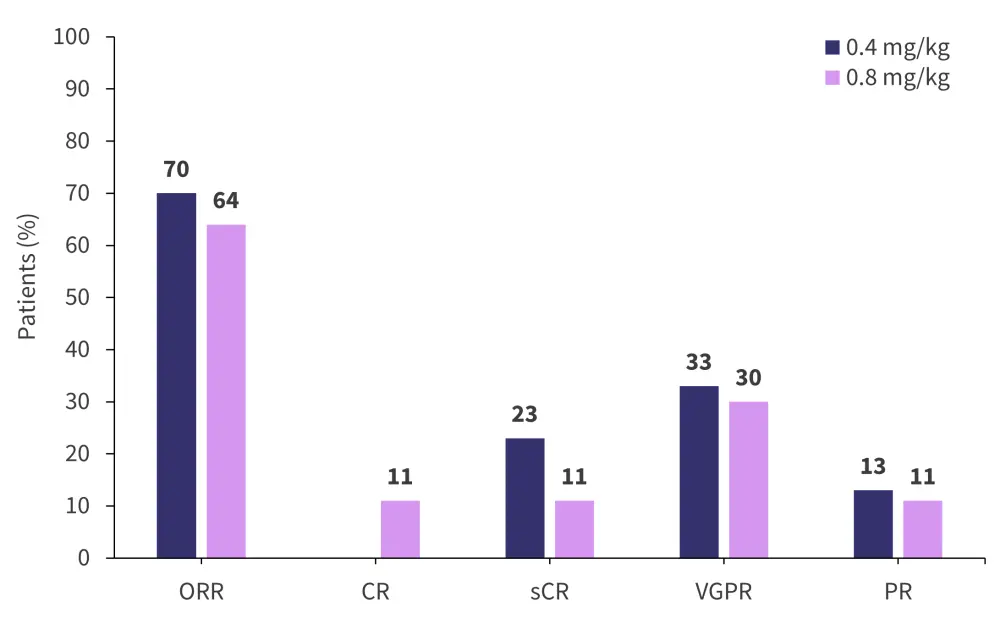
CR, complete response; ORR, overall response rate; PR, partial response; sCR, stringent complete response; VGPR, very good partial response.
*Adapted from Chari, et al.1
The most common adverse events (AEs) of any grade at the 0.4 mg/kg dose level were anemia and neutropenia at 60% and 67%, respectively. Likewise, the most common AEs of any grade for 0.8 mg/kg were anemia and neutropenia at 43% and 36%, respectively. Rates of any grade cytokine release syndrome for the 0.4 mg/kg dose and 0.8 mg/kg dose were 77% and 80%, respectively. The rate of any grade infection for 0.4 mg/kg was 47% and 34% for 0.8 mg/kg.
Combined analysis of phase I and II2
The final response rates for the combined analysis of patients treated with 0.4 mg/kg and 0.8 mg/kg of talquetamab in both the phase I and II parts of the trial are shown in Figure 2.
Figure 2. Combined response rates of patients treated with 0.4 mg/kg and 0.8 mg/kg of talquetamab from phases I and II*
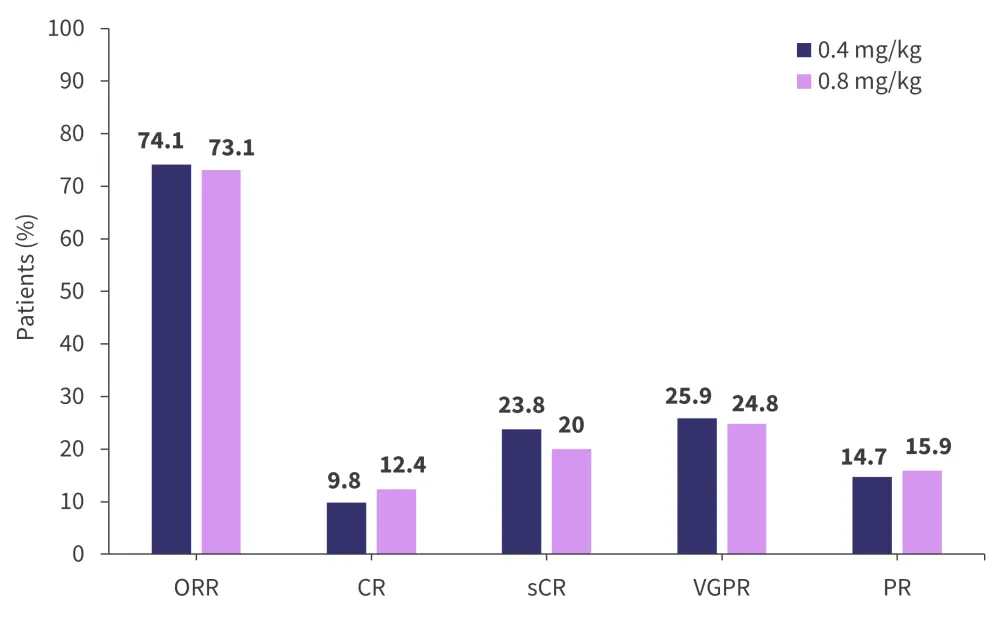
CR, complete response; ORR, overall response; PR, partial response; sCR, stringent complete response; VGPR, very good partial response.
*Adapted from Chari.2
The overall response rate was similar in both the 0.4 mg/kg and 0.8 mg/kg cohorts and was consistent across subgroups:
- Triple-class refractory: 72.6% and 71.0%, respectively
- Penta-class refractory: 71.4% and 70.6%, respectively
The median time to first response with the 0.4 mg/kg and 0.8 mg/kg doses was 1.2 months and 1.3 months, respectively. The median time to best response with the 0.4 mg/kg and 0.8 mg/kg doses was 2.2 months and 2.7 months, respectively.
Most high-grade AEs were cytopenias but were generally limited to the first treatment cycle. The most common AEs of Grade 3 or 4 in ≥20% of patients at both dose levels are summarized in Table 1 and the most common AEs of any grade in the entire cohort are presented in Table 2.
Table 1. Most common AEs in ≥20% of patients at both dose levels*
|
AE, adverse event; CRS, cytokine release syndrome. |
||
|
Most common Grade 3 or 4 AEs in ≥20% of patients, % |
0.4 mg/kg |
0.8 mg/kg |
|---|---|---|
|
Anemia |
31.5 |
24.8 |
|
Neutropenia |
30.8 |
22.1 |
|
Lymphopenia |
25.9 |
25.5 |
|
Thrombocytopenia |
20.3 |
16.6 |
|
Most common AEs of any grade in ≥20% of patients, % |
||
|
CRS |
79.0 |
72.4 |
|
Skin-related |
55.9 |
67.6 |
|
Nail-related |
51.7 |
43.4 |
|
Dysgeusia |
48.3 |
46.2 |
|
Rash-related |
39.2 |
26.9 |
The rate of any grade infection at the 0.4 mg/kg dose level was 57.3% compared with 50.3% for the 0.8 mg/kg dose level. Overall, there were low rates of Grade 3 or 4 non-hematologic AEs and only treatment discontinuation in 4.9% of patients treated at 0.4 mg/kg and 6.2% treated at 0.8 mg/kg. No deaths were reported due to drug-related AEs.
MonumenTAL-33
MonumenTAL-3 is an ongoing phase III trial (NCT05455320) of talquetamab + daratumumab ± pomalidomide compared with daratumumab + pomalidomide + dexamethasone in patients with R/R MM who had received ≥1 prior line of therapy. The study is currently recruiting patients with a target enrolment of 810 patients globally and will be randomized at a 1:1:1 ratio. The eligibility criteria are as follows:
- Measurable and progressive disease
- ≥18 years old
- Eastern Cooperative Oncology Group performance status 0–2
- Must have received ≥1 prior line of therapy including a proteasome inhibitor and lenalidomide
The primary endpoint is progression-free survival defined by the International Myeloma Working Group. Secondary endpoints include efficacy, biomarkers analysis, safety, and patient-reported outcomes.
MonumenTAL-54
MonumenTAL-5 is an ongoing phase III trial (NCT05461209) of talquetamab monotherapy versus belantamab mafodotin in patients with R/R MM who have previously had ≥4 lines of therapy. The study is currently recruiting patients with a target enrollment of 216 patients and the eligibility criteria are as follows:
- ≥18 years old
- Measurable disease
- Eastern Cooperative Oncology Group performance status 0–2
- ≥4 lines of prior therapy
- Progressive disease on or after last regimens
The primary objective is to investigate the efficacy and safety of talquetamab monotherapy versus belantamab mafodotin in patients with R/R MM.
Patients will be randomized at a 1:1 ratio for treatment with either 0.8 mg/kg of talquetamab every 2 weeks or 2.5 mg/kg of belantamab mafodotin every 3 weeks. The primary endpoint of the trial is overall response rate and progression-free survival. Secondary endpoints include overall survival, complete response, and very good partial response or better. Enrollment for the study began in October 2022.
Conclusion
Combined results from the phase I and II parts of the MonumenTAL-1 study highlight the overall promising efficacy with a manageable safety profile of talquetamab at both dosing levels in heavily pretreated patients with R/R MM. This has presented a rationale for further investigation, as shown by the prospective phase III trials currently in the stage of enrollment.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content