All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit the International Myeloma Foundation or HealthTree for Multiple Myeloma.
The Multiple Myeloma Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the Multiple Myeloma Hub cannot guarantee the accuracy of translated content. The Multiple Myeloma Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The Multiple Myeloma Hub is an independent medical education platform, sponsored by Abbvie, Roche, Bristol Myers Squibb, Pfizer, GSK, Johnson & Johnson, Legend Biotech and Caribou Biosciences. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account to access:
Bookmark & personalize site content
Receive alerts for new content in your areas of interest
View multiple myeloma content recommended for you
Strategies for managing belantamab mafodotin-associated ocular toxicities
 Heinz Ludwig
Heinz Ludwig Miles Prince
Miles Prince Rakesh Popat
Rakesh PopatDo you know... According to pooled analyses from the DREAMM-7 and DREAMM-8 studies, what was the approximate median time to resolution of the first Grade ≥2 ocular event associated with belantamab mafodotin?
During the Multiple Myeloma Hub Steering Committee Meeting on May 12, 2026, key opinion leaders met to discuss strategies for managing belantamab mafodotin-associated ocular toxicities in patients with multiple myeloma (MM). The meeting featured a presentation by guest speaker Lisa Leypoldt, University Medical Center Hamburg-Eppendorf, followed by a faculty discussion on the practical challenges of monitoring, managing, and counseling patients receiving belantamab mafodotin-based therapies.
Strategies for managing belantamab mafodotin-associated ocular toxicities
Strategies for managing belantamab mafodotin-associated ocular toxicities
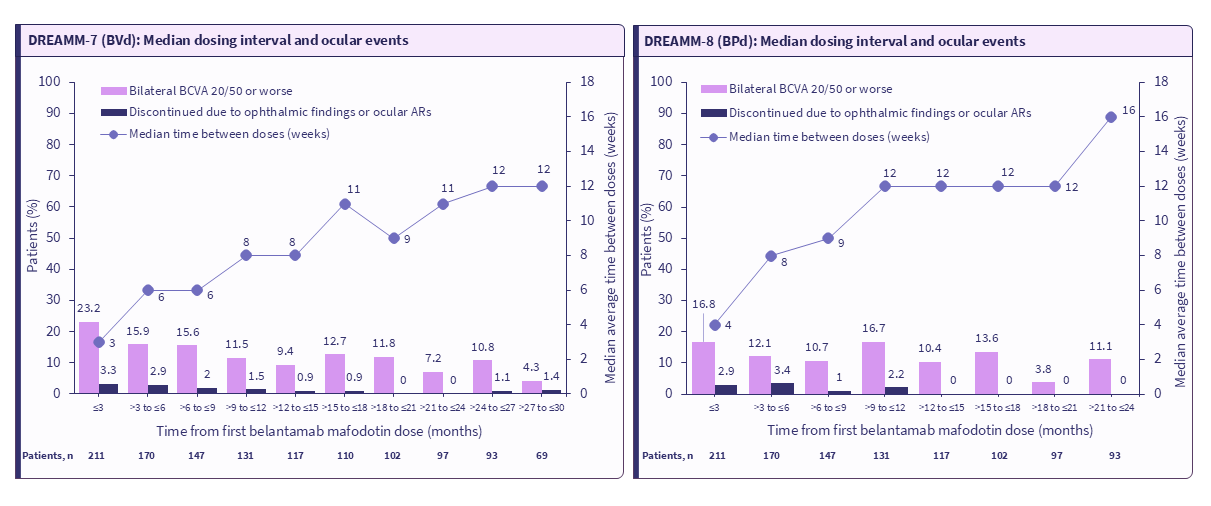
During their presentation, Leypoldt reviewed the mechanisms underlying belantamab mafodotin-associated ocular toxicity, highlighting the role of off-target uptake into corneal epithelial cells and the resulting transient visual symptoms (Figure 1). Leypoldt discussed the clinical manifestations of ocular events, including keratopathy, changes in visual acuity, and patient-reported symptoms, before outlining evidence-based approaches to monitoring and management. Leypoldt also reviewed data from the DREAMM-7 (NCT04246047) and DREAMM-8 (NCT04484623) studies, evaluating the role of dose modifications and extended dosing intervals in managing ocular toxicity (Figure 2). The subsequent faculty discussion focused on multidisciplinary care, patient counseling, and practical considerations for integrating ocular toxicity monitoring into routine clinical practice.
Figure 1. Mechanism of ocular toxicity with belantamab mafodotin*
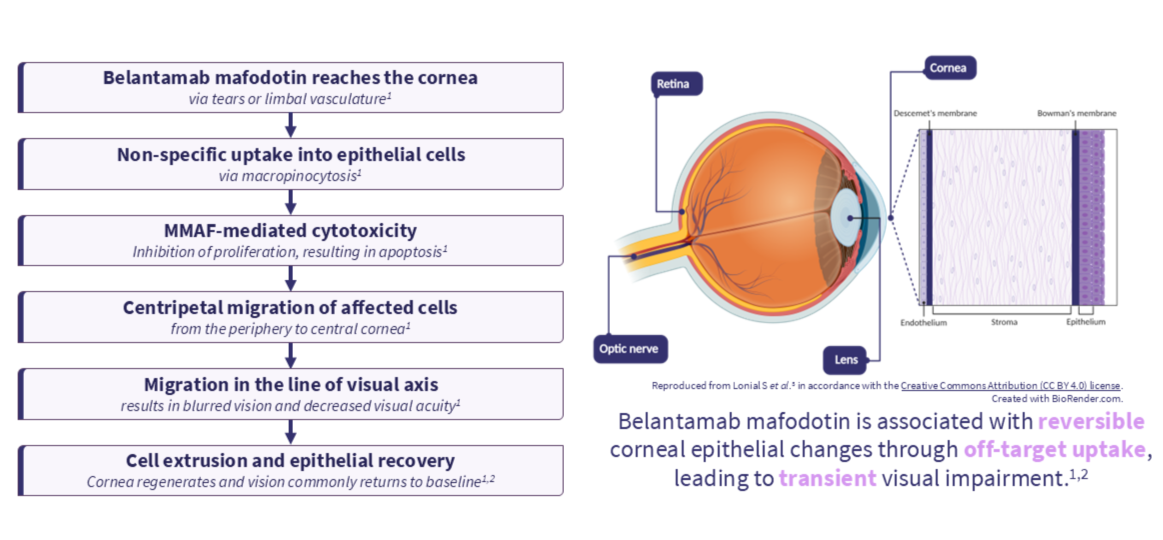
Figure 2. Impact of dose modifications on ocular toxicity*
Key learnings
- Belantamab mafodotin-associated ocular toxicity results from off-target uptake into corneal epithelial cells, leading to microcyst-like epithelial changes that may cause blurred vision and reduced visual acuity.1
- Ocular events associated with belantamab mafodotin are generally reversible, with recovery occurring through regeneration of the corneal epithelium.1,2
- Assessment of ocular toxicity should incorporate ophthalmic examination, visual acuity testing, and patient-reported symptoms, including the impact of visual changes on daily activities.5
- Baseline ophthalmologic evaluation and ongoing monitoring during early treatment cycles are important components of toxicity management.5
- Early identification and reporting of visual symptoms can facilitate timely intervention and support continued treatment.5
- Management of ocular toxicity commonly involves dose delays, treatment interruptions, and extension of dosing intervals based on the severity of ocular findings.4
- Data from the DREAMM-7 and DREAMM-8 studies demonstrate that dose modifications were frequently required in clinical practice, with dose delays occurring in most patients.4
- Extended dosing intervals were associated with a reduction in ocular events over time and allowed recovery from treatment-related ocular toxicity.
- Clinical responses were generally maintained despite extended dosing intervals.
- Effective management of ocular toxicity requires collaboration between hematology, ophthalmology, and primary care teams, with clear communication regarding monitoring findings and treatment decisions.
- Patient counseling should include discussion of expected visual symptoms, their potential impact on quality of life, the reversibility of ocular events, and the role of dose modifications in toxicity management.
This educational resource is independently supported by GSK. All content is developed by SES in collaboration with an expert steering committee. Funders are allowed no influence.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content


