All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit the International Myeloma Foundation or HealthTree for Multiple Myeloma.
The Multiple Myeloma Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the Multiple Myeloma Hub cannot guarantee the accuracy of translated content. The Multiple Myeloma Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The Multiple Myeloma Hub is an independent medical education platform, sponsored by Abbvie, Roche, Bristol Myers Squibb, Pfizer, GSK, Johnson & Johnson, Legend Biotech and Caribou Biosciences. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account to access:
Bookmark & personalize site content
Receive alerts for new content in your areas of interest
View multiple myeloma content recommended for you
EBMT 2024: Latest updates from CARTITUDE-2 and CARTITUDE-4
Ciltacabtagene autoleucel (cilta-cel), a BCMA-directed chimeric antigen receptor (CAR) T-cell therapy, is approved for the treatment of relapsed/refractory multiple myeloma (RRMM) after four or more prior lines of therapy, including a proteasome inhibitor, an immunomodulatory agent, and an anti-CD38 monoclonal antibody. Cilta-cel is currently under investigation as part of the CARTITUDE trials for expanding indications in MM and impact on patient-reported outcomes (PROs).
Here, we summarize presentations by Tessa Kerre and Roberto Mina from the 50th Annual Meeting of the European Society for Blood and Marrow Transplantation (EBMT) on the latest data from CARTITUDE-2 and CARTITUDE-4, respectively.
CARTITUDE-21
Study design
The phase II CARTITUDE-2 trial (NCT04133636) evaluated the safety and efficacy of cilta-cel in:
- patients with 1–3 prior lines of therapy (cohort A; n = 20);
- patients with 1 prior line of therapy who relapsed ≤12 months after transplant or antimyeloma treatment initiation (cohort B; n = 19); and
- the primary endpoint was negative measurable residual disease (MRD) at a sensitivity of 10−5.
Results
- The majority of patients experienced MRD negativity after treatment in both cohorts, with ≥50% achieving sustained MRD negativity at 12 months (Table 1).
- Overall response was higher in cohort B (Figure 1).
- Efficacy rates were largely comparable between cohorts A and B at 24 months posttreatment initiation (Table 1).
- In both cohorts, hematologic treatment-emergent adverse events were most common, with neutropenia occurring in approximately 95% of patients in both cohorts; almost all events were Grade 3/4.
- Cytokine release syndrome was common in both cohorts, at 95% and 84.2% in cohorts A and B, respectively, with the majority Grade 1/2 and able to be resolved.
Table 1. Efficacy data from CARTITUDE-2*
|
CR, complete response; DoR, duration of response; MRD, measurable residual disease; OS, overall survival; PFS, progression-free survival. |
||
|
Outcome, % (unless otherwise specified) |
Cohort A |
Cohort B |
|---|---|---|
|
MRD negativity ×10−5 |
100 |
93.3 |
|
Sustained MRD negativity ×10−5 at ≥12 months |
50 |
61.5 |
|
MRD in ≥CR |
85 |
68.4 |
|
24-month DoR rate |
73.3 |
70.5 |
|
24-month PFS rate |
75 |
73 |
|
24-month OS rate |
75 |
84 |
Figure 1. Response rates in cohort A and B from CARTITUDE-2*
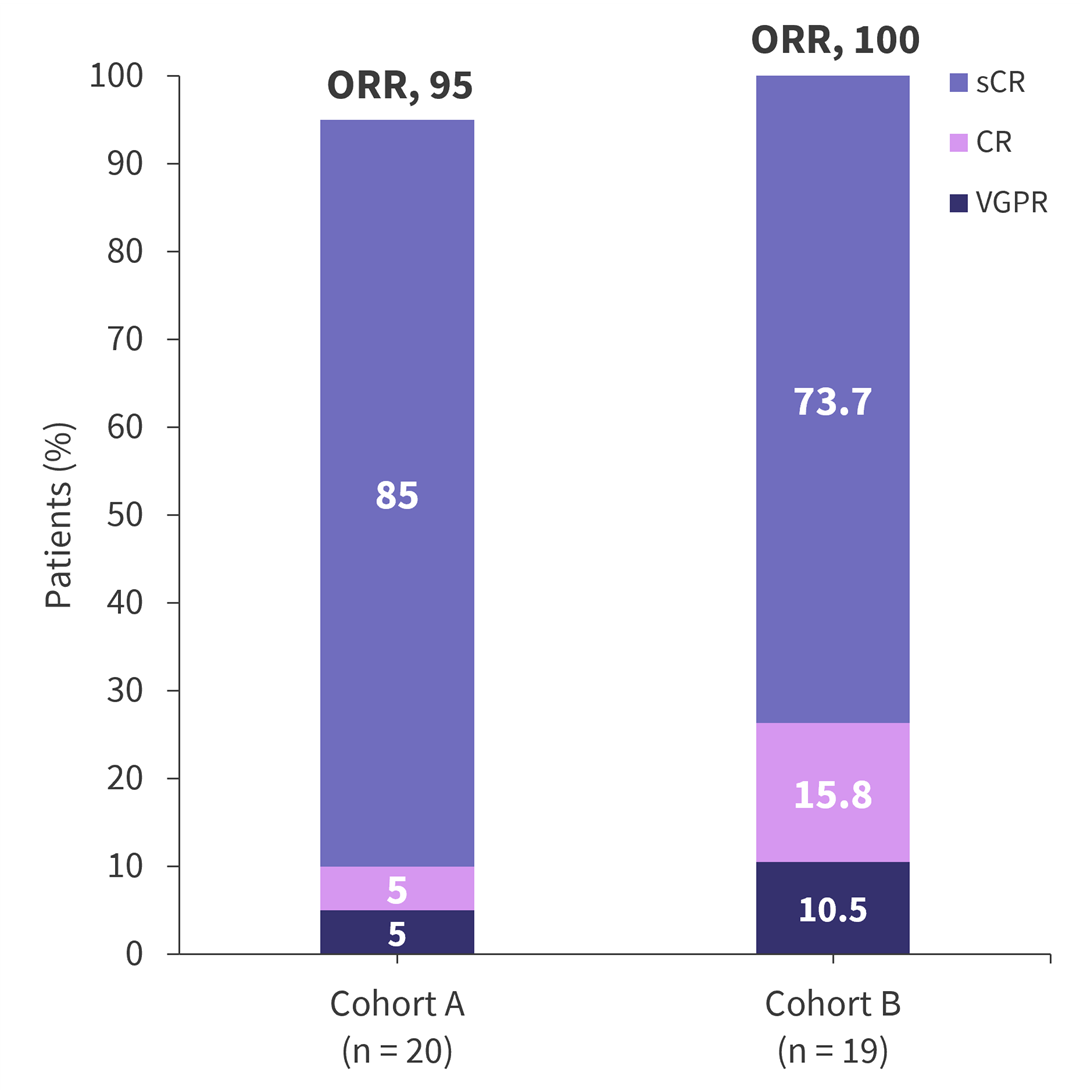
CR, complete response; ORR, overall response rate; sCR, stringent complete response; VGPR, very good partial response.
*Adapted from Kerre.1
CARTITUDE-42
Study design
- The phase III CARTITUDE-4 (NCT04181827) trial evaluated the safety and efficacy of cilta-cel in patients with lenalidomide-refractory MM after 1–3 prior lines of therapy (n = 99) versus a standard of care (SoC) regimen (n = 66).
- The primary endpoint was progression free survival.
Results
- Baseline PROs were largely comparable between cohorts.
- Global health status (GHS) improved in the cilta-cel arm by the end of the follow-up period but not in the SoC arm (Figure 2)
- A least squares mean change from baseline in GHS of 10.1 was recorded in the cilta-cel arm vs −1.5 points in the SoC arm.
- In the European Organization for the Research and Treatment of Cancer Quality of Life Questionnaire, improvements were largely observed in the cilta-cel arm, with the sole improvement in the SoC arm being emotional functioning (Table 2).
- Improvements in pain and fatigue were also observed in the cilta-cel arm compared with the SoC arm, with improvements in 51.5% and 54.6% of patients, respectively.
Figure 2. Clinically meaningful change in global health status at 12 months*
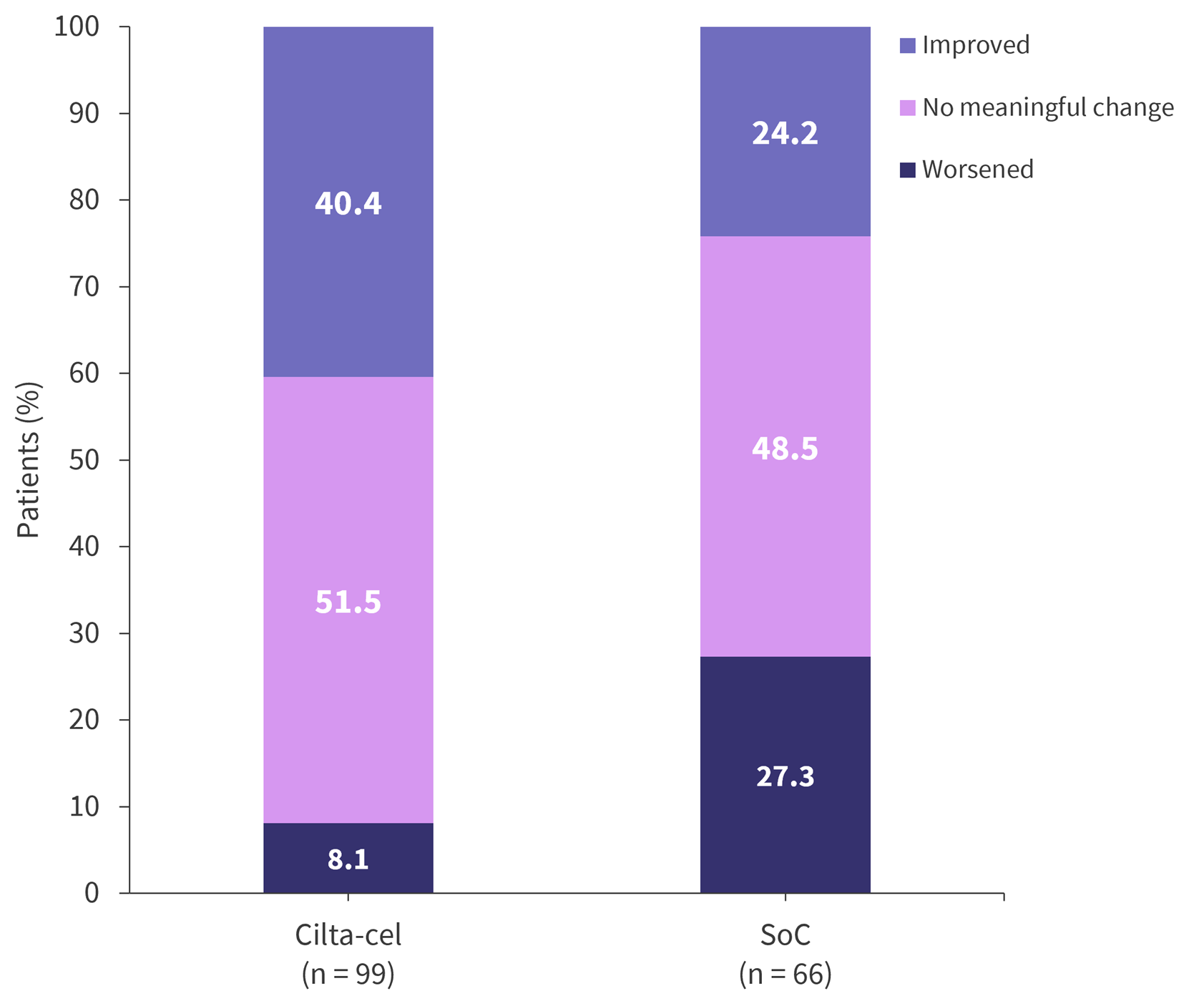
*Adapted from Mina.2
Table 2. EORTC QLQ-C30 LS mean change from baseline to Month 12*
|
cilta cel, ciltacabtagene autoleucel; LS, least squares; SoC, standard of care. |
||
|
Functional scale |
LS mean change from baseline |
|
|---|---|---|
|
Cilta-cel (n = 99) |
SoC (n = 66) |
|
|
Cognitive |
0.5 (−2.4, 3.5) |
−7.5 (−11.2, −3.9) |
|
Emotional |
9.5 (6.6, 12.5) |
2.2 (−1.3, 5.7) |
|
Physical |
6.5 (3.8, 9.1) |
−2.1 (−5.0, 0.7) |
|
Role |
7.7 (3.7, 11.7) |
−1.7 (−6.3, 2.9) |
|
Social |
6.1 (2.1, 10.0) |
−0.1 (−4.2, 4.0) |
|
Key learnings1,2 |
|---|
|
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content


