All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit the International Myeloma Foundation or HealthTree for Multiple Myeloma.
The Multiple Myeloma Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the Multiple Myeloma Hub cannot guarantee the accuracy of translated content. The Multiple Myeloma Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The Multiple Myeloma Hub is an independent medical education platform, sponsored by Bristol Myers Squibb, GSK, Johnson & Johnson Innovative Medicine, Legend Biotech, Pfizer, Roche, and Caribou Biosciences. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account to access:
Bookmark & personalize site content
Receive alerts for new content in your areas of interest
View multiple myeloma content recommended for you
Symposium | How to sequence CAR T-cell therapy and bispecific antibodies in relapsed/refractory multiple myeloma
Featured:
 Sagar Lonial
Sagar LonialDo you know... In a real-world study by Dima et al. in 2023, which type of prior BCMA-directed therapy was associated with the highest response to subsequent teclistamab therapy in patients with relapsed/refractory multiple myeloma?
During the European Hematology Association (EHA) 2024 Hybrid Congress, the Lymphoma Hub and Multiple Myeloma Hub held a joint satellite symposium entitled ‘Sequencing immune-based therapies in B-cell malignancies’. Here, the Multiple Myeloma Hub is pleased to share the session, which covered how to sequence CAR T-cell therapy and bispecific antibodies in relapsed/refractory (R/R) multiple myeloma (MM), presented by Sagar Lonial, Winship Cancer Institute of Emory University, Atlanta, US.
Symposium | How to sequence CAR T-cell therapy and bispecific antibodies in relapsed/refractory multiple myeloma
Listen to the podcast here:
Q&A | How to sequence CAR T-cell therapy and bispecific antibodies in R/R MM
In this presentation, Lonial began by reviewing the current landscape for the treatment of early relapse in lenalidomide-refractory myeloma using data from ICARIA, CANDOR, IKEMA, APOLLO, and MM-014 trials. 1
Lonial then discussed the key considerations for sequencing, namely to maximize short-term response, maximize subsequent therapy, and through both of these to improve overall progression-free survival (PFS) and overall survival (OS). He started by questioning, ‘What does resistance to BCMA mean?’ As part of this discussion, he provided an overview of the mechanism of action of T-cell engagers (Figure 1) and immunotherapy treatment failure in MM (Figure 2).
Figure 1. T-cell engagement in multiple myeloma*
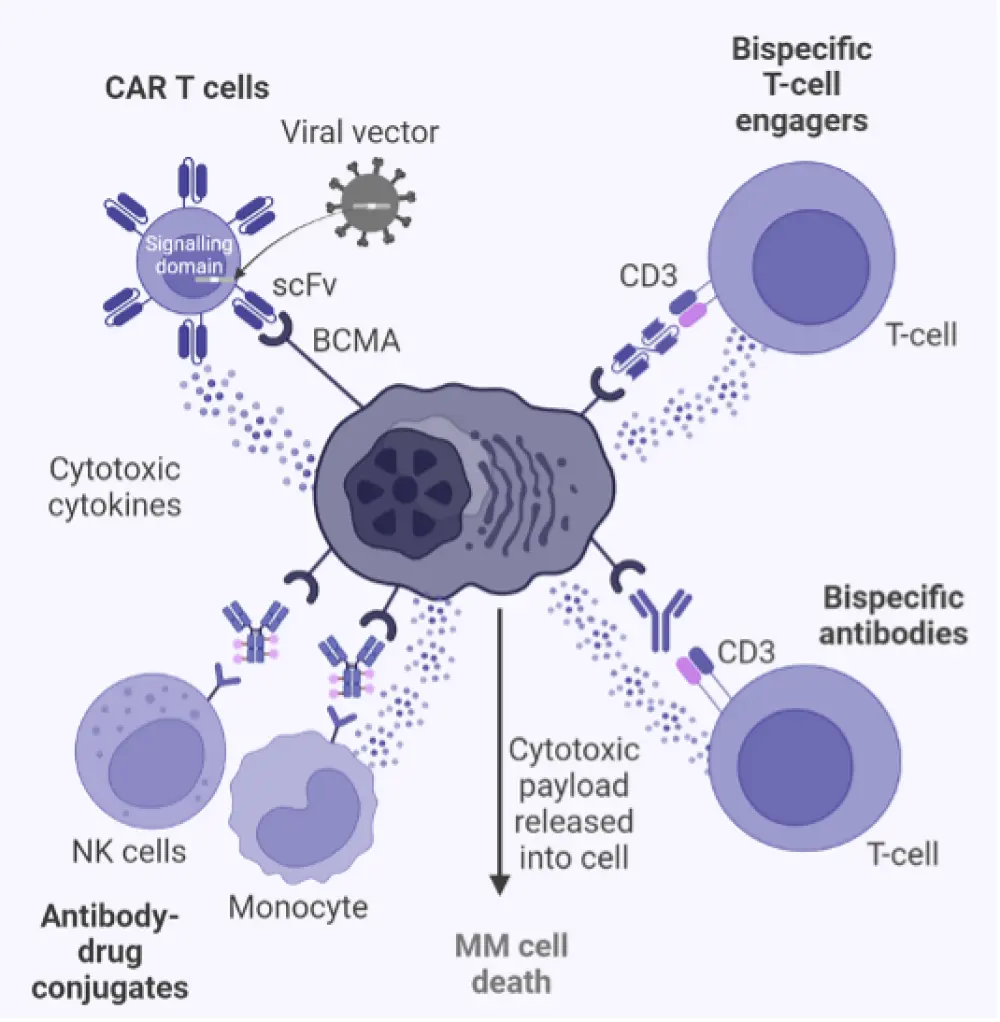
BCMA, B-cell maturation antigen; CAR, chimeric antigen receptor; MM, multiple myeloma; NK, natural killer; R/R, relapsed/refractory; scFv, single-chain fragment variable.
*Created with BioRender.com.
Figure 2. Immunotherapy treatment failure in multiple myeloma
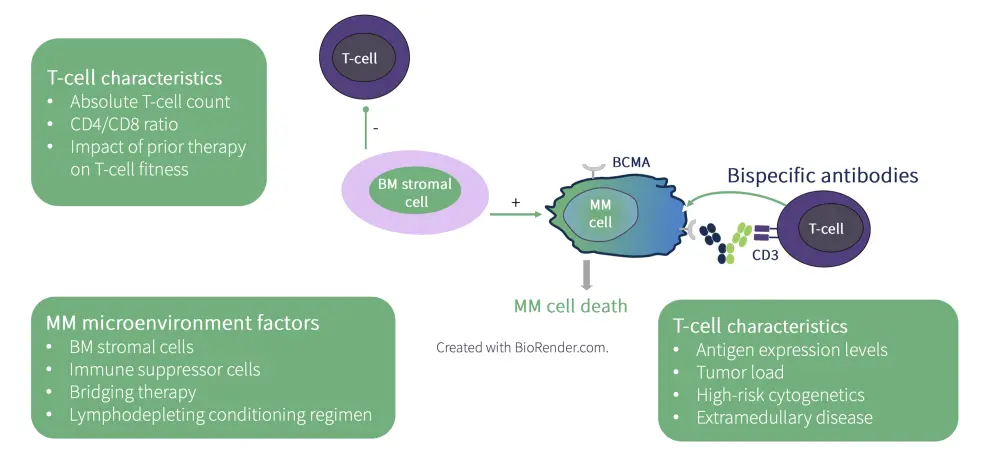
BCMA, B-cell maturation antigen; BM, bone marrow; MM, multiple myeloma.
*Adapted from Van de Donk N, et al.5
Lonial shared the currently approved CAR T-cell therapy and bispecific antibodies for MM (Table 1) and discussed the latest clinical data for sequencing these agents.
Table 1. FDA-approved CAR T-cell therapy and bispecific antibodies for R/R MM*
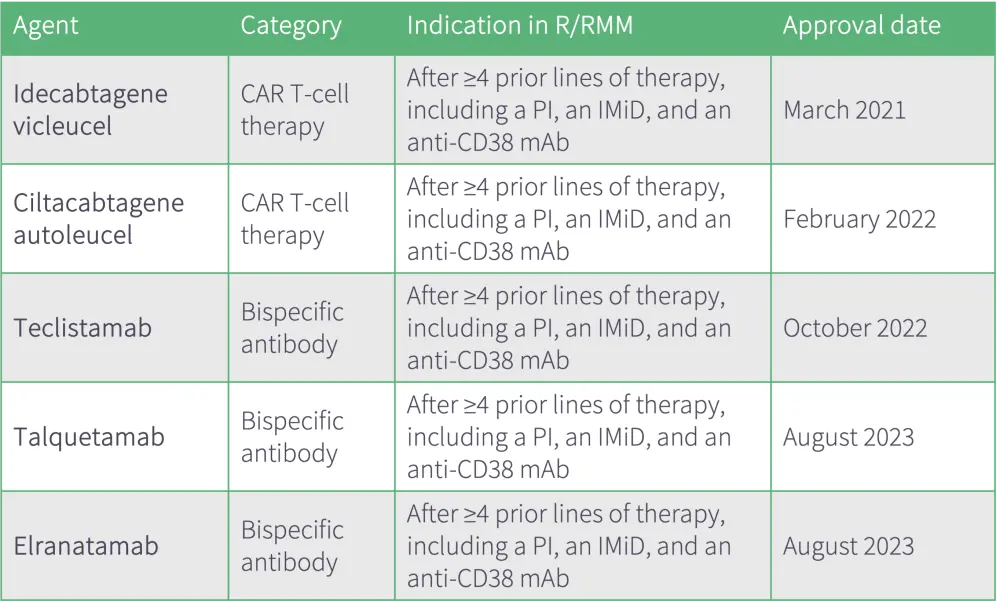
CAR, chimeric antigen receptor; IMiD, immunomodulatory agent; mAb, monoclonal antibody; MM, multiple myeloma; PI, proteosome inhibitor; R/R, relapsed/refractory; TCE, T-cell engager.
*Data adapted from FDA. Development & approval process.6
Watch or download the presentation to learn more about:
- the myeloma treatment landscape;
- the currently approved CAR T-cell products and bispecifics in multiple myeloma, including their up-to-date safety and efficacy data; and
- the impact of prior treatment with BCMA therapy on clinical outcomes with CAR T-cell therapy and anti-BCMA bispecific antibodies.
Key points
The efficacy of anti-BCMA bispecific antibodies after prior BCMA therapy was comparable to the efficacy observed in BCMA-naïve patients.
- In a phase I/II study, treatment with elranatamab, after previous BCMA therapy, showed that patients who started elranatamab who previously received CAR T-cell treatment had a numerically higher ORR and PFS vs patients who previously received any BCMA or antibody-drug conjugate (ADC) treatment.
- Analysis of real-world teclistamab response by prior BCMA-directed therapy showed that patients who received ADC plus CAR T-cell therapy prior to BCMA-directed therapy had the highest response to subsequent teclistamab therapy (ORR = 80%) compared with those who received prior antibody-drug conjugate (ORR, 50%), CAR T-cell therapy (ORR, 57%), or antibody-drug conjugate plus other treatment (ORR, 33%).
Prior BCMA-directed therapy influences response to CAR T-cell therapy.
- In the CARTITUDE-2 study, the timing of prior anti-BCMA therapy affected responses to ciltacabtagene autoleucel following BCMA-targeted therapy.
- In an analysis of real-world outcomes with idecabtagene vicleucel post-BCMA-targeted therapy, patients with no prior BCMA targeted therapy had higher PFS vs patients with any prior BCMA-targeted therapy.
- According to a multivariable analysis of idecabtagene vicleucel post-BCMA-targeted therapy, Eastern Cooperative Oncology Group Performance Status ≥2, high risk cytogenetics, and prior BCMA-targeted therapy were associated with inferior PFS and OS.
- In a phase I study, treatment with talquetamab in patients with prior exposure to the T-cell redirection therapy showed that patients with prior treatment with CAR T-cell therapy achieved a higher ORR compared with patients who have had prior treatment with bispecific antibody (72.2% vs 44.4%, respectively)
In conclusion, optimal sequencing may be to use a CAR T-cell therapy first to maximize first remission, then to utilize a different target before returning to a BCMA T-cell engager. Ultimately, the mechanism of failure will be important to understand.
Q&A
This symposium closed with a panel Q&A session with live audience participation, where our panelists shared their perspectives on how to sequence CAR T-cell therapy and bispecific antibodies in R/R MM.
Q&A | How to sequence CAR T-cell therapy and bispecific antibodies in R/R MM
This independent educational activity was supported by Bristol Myers Squibb. All content was developed independently by the faculty. The funder was allowed no influence on the content of this activity.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content