All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit the International Myeloma Foundation or HealthTree for Multiple Myeloma.
The Multiple Myeloma Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the Multiple Myeloma Hub cannot guarantee the accuracy of translated content. The Multiple Myeloma Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The Multiple Myeloma Hub is an independent medical education platform, sponsored by Bristol Myers Squibb, GSK, Johnson & Johnson Innovative Medicine, Legend Biotech, Pfizer, Roche, and Caribou Biosciences. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account to access:
Bookmark & personalize site content
Receive alerts for new content in your areas of interest
View multiple myeloma content recommended for you
Predicting early relapse in patients with multiple myeloma
Although emerging novel agents have improved patient survival outcomes significantly, early relapse (ER) remains an area of unmet clinical need in the multiple myeloma (MM) setting. There have been a number of attempts to better characterize patients who relapse: at the 25th European Hematology Association (EHA) Annual Congress, three posters outlined the latest advancements achieved by GIMEMA and the European Myeloma Network in Italy, in predicting ER and survival outcomes for patients with MM. The Multiple Myeloma Hub is pleased to provide a summary.
Simplified early relapse in multiple myeloma (S-ERMM) score1
Gian Maria Zaccaria and colleagues aimed to design a predictive model and scoring system to define patients who will likely relapse within 18 months of diagnosis (ER18). The team hoped to correlate the simplified early relapse in multiple myeloma (S-ERMM) score with overall survival (OS) and progression-free survival until the second relapse (PFS2).
Below you will find a summary of how the authors created and validated this model, but you can calculate the S-ERMM score here: sermm.emnitaly.org/.
Study design
- Patient data from seven clinical trials (N = 2,190; NCT01093196, NCT01346787, NCT01857115, NCT01190787, NCT00551928, NCT01091831, NCT02203643) with 14 distinct clinical features (Table 1) were pooled
- Multivariate analyses and OS landmark analysis were undertaken to define low-, medium-, and high-risk ER
- The S-ERMM model was constructed using this survival analysis
- The established model was validated in an independent study (FORTE trial, NCT02203643)
Results
- Of the 2,190 patient data sets, 1,218 were complete and eligible for the analysis. These patients subsequently comprised the training and validation cohorts (Table 1)
Table 1. Baseline characteristics of patients eligible for ER18 analysis vs reference population (late relapse or death without progression after 18 months)1
|
B2M, beta 2 microglobulin; CA, chromosomal abnormality; ER18, early relapse (within 18 months of diagnosis); FLC, free light chain; IgA, immunoglobulin A; IQR, interquartile range; LDH, lactate dehydrogenase; PCbm, plasma-cells bone marrow; R-ISS, Revised International Staging System; ULN, upper limit of normal |
||||||
|
Features |
Training cohort (n = 844) |
Validation cohort (n = 374) |
||||
|
|
ER18 (n = 312) |
Reference (n = 532) |
p |
ER18 (n = 61) |
Reference (n = 313) |
p |
|
Median age, years (IQR) |
68 (58–75) |
65 (57–73) |
0.03 |
56 (48—62) |
58 (52–62) |
0.17 |
|
Median albumin, g/dL (IQR) |
3.7 (3.2–4.1) |
3.9 (3.5–4.2) |
< 0.01 |
3.7 (3.4–4.1) |
3.9 (3.5–4.3) |
0.05 |
|
LDH > ULN, % |
14 |
7 |
< 0.01 |
28 |
12 |
0.02 |
|
Presence of CAs, % |
|
|
|
|
|
|
|
Del(17p) |
19 |
12 |
< 0.01 |
18 |
13 |
0.38 |
|
t(4;14) |
20 |
10 |
< 0.01 |
28 |
13 |
0.04 |
|
t(11;14) |
16 |
20 |
0.19 |
23 |
13 |
1 |
|
t(14;16) |
5 |
3 |
0.17 |
6.6 |
5 |
0.77 |
|
R-ISS II/III, % |
82 |
67 |
< 0.01 |
87 |
63 |
< 0.01 |
|
PCbm > 60%, % |
36 |
25 |
< 0.01 |
44 |
36 |
0.26 |
|
FLC λ, % |
39 |
34 |
0.1 |
30 |
40 |
0.17 |
|
Plasmacytoma, % |
9 |
10 |
0.74 |
16 |
12 |
0.53 |
- Comparing both subgroups, ER18 vs reference population, the researchers identified six clinical features that significantly increased the risk of ER18 (Table 2) and were incorporated into the S-ERMM model (Table 3)
Table 2. Clinical features significantly and positively correlated with an increased risk of ER181
|
FLC, free light chain; LDH, lactate dehydrogenase; PCbm, plasma-cells bone marrow; ULN, upper limit of normal |
||
|
Variable |
Coefficient, β proportionality |
Score |
|
LDH > ULN |
2.4 |
5 |
|
Presence of t(4;14) |
2.6 |
5 |
|
Presence of del(17p) |
1.7 |
3 |
|
Abnormal albumin |
1.5 |
3 |
|
PCbm > 60% |
1.7 |
3 |
|
FLC λ |
1.0 |
2 |
Table 3. S-ERMM risk groups1
|
S-ERMM, simplified early relapse in multiple myeloma score |
|
|
Risk |
Score |
|
S-ERMM Low |
≤ 5 |
|
S-ERMM Intermediate |
6–10 |
|
S-ERMM High |
≥ 11 |
As demonstrated in Table 4, median OS, PFS2, and 4-year probability rates were significantly lower in patients classified as
-
- S-ERMM intermediate vs S-ERMM low
- S-ERMM high vs S-ERMM low
- S-ERMM high vs S-ERMM intermediate
Table 4. Patient OS and PFS2 rates with regard to S-ERMM characterization1
|
CI, confidence interval; NR, not reached; OS, overall survival; PFS2, progression-free survival until second relapse |
||||||
|
|
OS |
PFS2 |
||||
|
S-ERMM characterization |
Low (n = 574) |
Intermediate (n = 214) |
High (n = 56) |
Low (n = 574) |
Intermediate (n = 214) |
High (n = 56) |
|
Events |
204 |
117 |
40 |
302 |
150 |
47 |
|
Median, months |
NR |
59.5 |
31.5 |
62.3 |
40.0 |
19.8 |
|
95% CI |
83–NR |
50.5–74.2 |
23–53.5 |
54.6–69.7 |
33.7–46.5 |
16.6–30.7 |
|
4-year probability |
0.75 |
0.59 |
0.35 |
0.60 |
0.40 |
0.22 |
|
95% CI |
0.72–0.79 |
0.52–0.66 |
0.24–0.51 |
0.55–0.64 |
0.33–0.47 |
0.13–0.36 |
Study conclusions
- Three distinct S-ERMM categories of patients were identified as being able to assess the risk of relapse within 18 months from diagnosis, and identify effectively those patients with a higher risk in order to plan therapy strategy and follow-up accordingly
Circulating plasma cells and sustained measurable residual disease negativity2
Poor patient survival outcomes have been associated with elevated levels of circulating plasma cells (CPCs). Luca Bertamini and colleagues aimed to determine the relationship between CPC levels at the time of MM diagnosis and sustained measurable residual disease (MRD) negativity (≥ 12 months; MRDsus12), and to identify clinical features that could couple with both variables in patients enrolled on the FORTE/UNITO-MM1 trial (NCT02203643).
Study design
- Patients enrolled on the FORTE trial (N = 474) were assessed for
- pre-maintenance MRD
- 6-month periodical MRD
- MRDsus12
- CPC at diagnosis (% and absolute count determined using flow cytometry)
- Eligible patients comprised two study cohorts:
- Cohort 1: All patients evaluated for MRDsus12 (n = 390)
- Cohort 2: Of these, patients presenting CPC at baseline who were evaluated for MRDsus12 (n = 328; median follow-up, 34.4 months)
Results
- CPC cut-offs for cohort 2 were defined as
- low CPC: ≤ 0.07%
- high CPC: > 0.07%
- A number of clinical features differed significantly between high and low CPC readouts (Table 5)
- Favorable MRDsus12 rates were associated with low CPC, and differed between treatment regimens (Figure 1)
Table 5. Clinical features associated with CPC levels at the time of MM diagnosis in patients from cohort 22
|
CPC, circulating plasma cells; FISH, fluorescence in situ hybridization; ISS, International Staging System; LDH, lactate dehydrogenase; PCbm, plasma-cells bone marrow; R-ISS, Revised ISS; ULN, upper limit of normal |
|||
|
Feature, % |
Low CPC (n = 220) |
High CPC (n = 108) |
p |
|
ISS |
|
|
|
|
I |
62 |
30 |
< 0.001 |
|
II |
27 |
41 |
|
|
III |
10 |
30 |
|
|
FISH |
|
|
|
|
Standard risk |
74 |
51 |
< 0.001 |
|
High risk |
26 |
49 |
|
|
del(17p) |
11 |
24 |
0.006 |
|
del(13) |
44 |
67 |
< 0.001 |
|
t(14;16) |
2 |
12 |
0.001 |
|
amp(1q) |
42 |
59 |
0.006 |
|
LDH > ULN |
9 |
24 |
< 0.001 |
|
R-ISS |
|
|
|
|
I |
40 |
12 |
< 0.001 |
|
II |
56 |
71 |
|
|
III |
4 |
17 |
|
|
PCbm (> 60%) |
26 |
50 |
< 0.001 |
Figure 1. MRDsus12 rates2
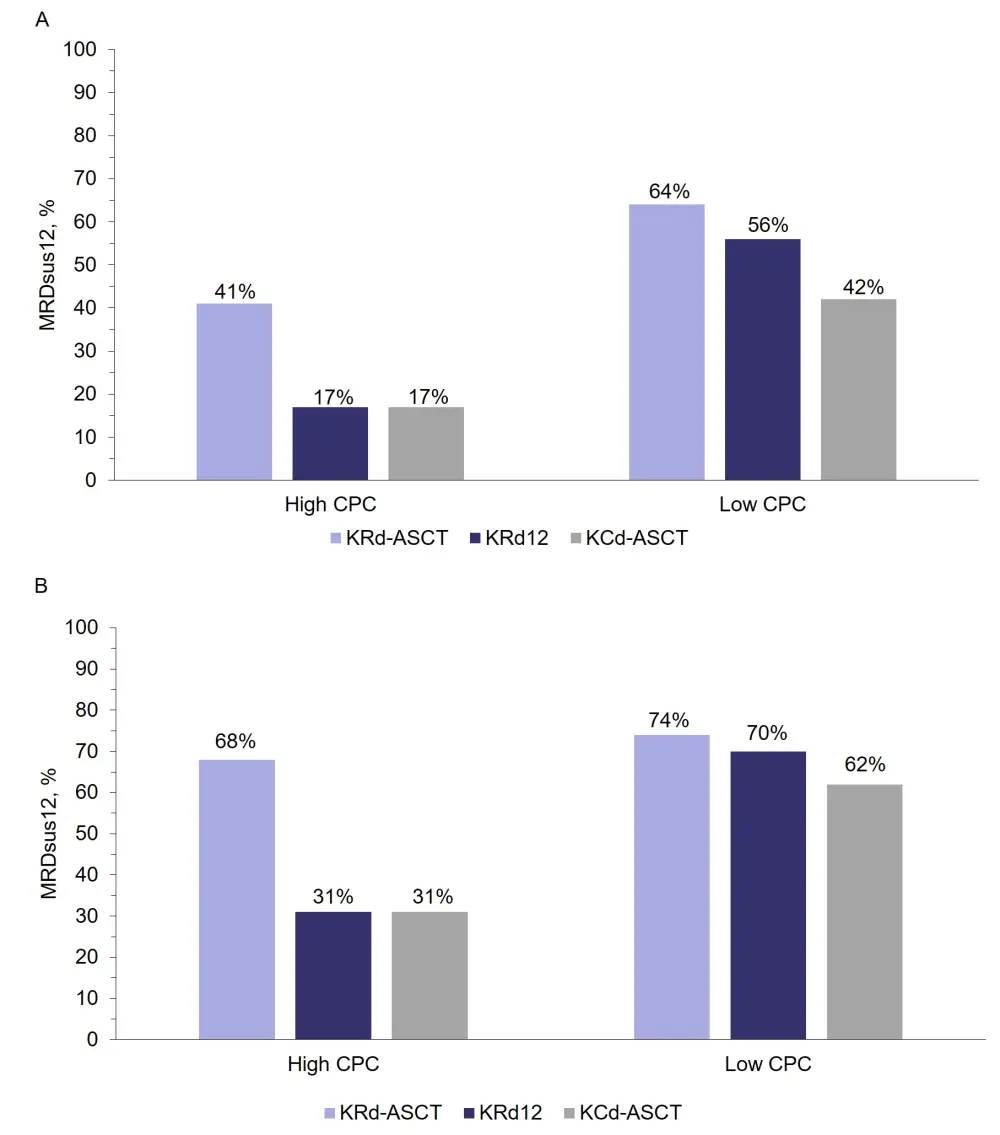
A MRDsus12 rates including all eligible patients (cohort 2), and B MRDsus12 rates considering patients with MRD negativity only; analyzed according to high vs low CPC at time of MM diagnosis2
ASCT, autologous stem cell transplantation; CPC, circulating plasma cells; KCd, carfilzomib + cyclophosphamide + dexamethasone; KRd, carfilzomib + lenalidomide + dexamethasone; KRd12, 12 cycles of KRd; MRD, measurable residual disease, MRDsus12, sustained MRD negativity for ≥ 12 months
Study conclusions
- Several clinical features are associated with high CPC levels which, in turn, are considered to reduce the probability of achieving an MRDsus12
- Patients with high CPC who were treated with KRd-ASCT demonstrated superior MRDsus12 rates vs those treated with KRd12 or KCd-ASCT (Figure 1)
- Data from this study provide valuable information on independent factors contributing to ER, and additional tools to identify those patients at a higher risk, but longer-term analyses are required to consolidate these results
Validation of ER predictors—S-ERMM and MRD negativity3
A team led by Francesca Gay aimed to establish and strengthen the S-ERMM score as well as identify additional features that are associated with MRD negativity achievement and may predict ER18.
Study design
- Patients enrolled on the FORTE trial (N = 474) were included in multivariate analyses to determine baseline features associated with ER18 and MRD status
Results
- In patients receiving novel agents for the treatment of NDMM, predictors of MRD negativity and risk of ER18 were identified by multivariate analyses (Table 6)
Table 6. Clinical factors, other than therapy, that significantly impact MRD negativity rates and patient risk of ER183
|
CPC, circulating plasma cells; ER18, early relapse (within 18 months of diagnosis); ISS, International Staging System; MRD, measurable residual disease; PCbm, plasma cells in bone marrow; S-ERMM, simplified early relapse in multiple myeloma |
||
|
|
Odds ratio (95% CI) |
p |
|
Decreased MRD negativity |
|
|
|
ISS III vs ISS II |
0.50 (0.29–0.85) |
0.01 |
|
PCbm > 60% vs ≤ 60% |
0.65 (0.44–0.97) |
0.03 |
|
del(17p) present vs not present |
0.40 (0.22–0.72) |
< 0.001 |
|
Increased risk of ER18 |
|
|
|
S-ERMM |
|
|
|
Intermediate vs low |
1.93 (0.99–3.74) |
0.049 |
|
High vs low |
4.45 (1.68–11.72) |
< 0.001 |
|
CPC, > 0.13 vs ≤ 0.13 |
2.68 (1.38–5.20) |
< 0.001 |
|
Decreased risk of ER18 |
|
|
|
MRD negative vs MRD positive |
0.26 (0.14–0.48) |
< 0.001 |
Study conclusions
- This analysis validated S-ERMM as an accurate predictor of ER18
- CPC level at baseline was identified as an independent factor to predict ER18 and could be included in the S-ERMM model
- Achieving MRD negativity significantly reduces the risk of early relapse
- International Staging System (ISS)-III, PCbm ≥ 60%, and presence of del(17p) could help identify at diagnosis the patients that have a lower probability of achieving a deep response with therapy, and enable adaptation of a therapeutic strategy accordingly
Conclusion
Data from these studies provide a clearer understanding of the factors contributing towards ER in patients with MM. The combination of the S-ERMM system with other ER contributors may pave the way towards risk-adaptive treatment regimens.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content