All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit the International Myeloma Foundation or HealthTree for Multiple Myeloma.
The Multiple Myeloma Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the Multiple Myeloma Hub cannot guarantee the accuracy of translated content. The Multiple Myeloma Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The Multiple Myeloma Hub is an independent medical education platform, sponsored by Bristol Myers Squibb, GSK, Johnson & Johnson Innovative Medicine, Legend Biotech, Pfizer, Roche, and Caribou Biosciences. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account to access:
Bookmark & personalize site content
Receive alerts for new content in your areas of interest
View multiple myeloma content recommended for you
Integrating BCMA-directed bispecific antibodies into the treatment paradigm for MM
Featured:
 Heinz Ludwig
Heinz Ludwig Miles Prince
Miles Prince Rakesh Popat
Rakesh PopatDo you know... According to the IMWG consensus, which of the following factors may favor the use of a BCMA-directed bispecific antibody over CAR T-cell therapy?
During the Multiple Myeloma Hub Steering Committee Meeting on May 12, 2026, key opinion leaders met to discuss the integration of B-cell maturation antigen (BCMA)-directed bispecific antibodies (BsAbs) into the treatment paradigm for multiple myeloma (MM). The discussion was led by Miles Prince (Peter MacCallum Cancer Centre, Melbourne, AU) and featured steering committee members Rakesh Popat and Heinz Ludwig. The discussion explored key considerations for patient selection, treatment sequencing, and implementation of BsAb therapy in clinical practice.
Integrating BCMA-directed bispecific antibodies into the treatment paradigm for MM
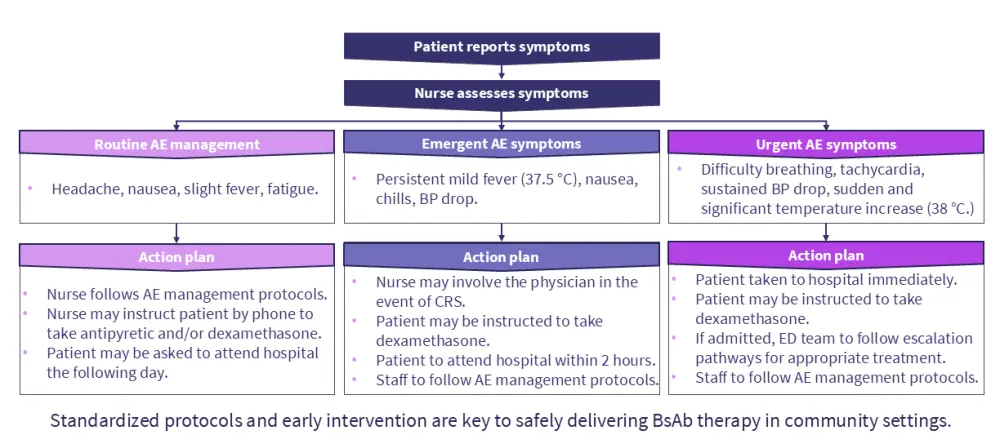
Prince reviews the currently approved BCMA-directed BsAbs and key factors influencing treatment selection, including disease burden, prior therapy, T-cell fitness, patient preferences, and treatment access. Prince also discusses emerging treatment strategies, including combination regimens and earlier-line use of BsAbs, before exploring practical considerations related to dosing, toxicity management, and community-based treatment delivery (Figures 1 and 2). The subsequent discussion focused on expanding access to BsAb therapy, the role of standardized toxicity management pathways, and challenges associated with transitioning patients from specialist centers to community-based care.
Figure 1. Transitioning BCMA-directed BsAbs to community practice*
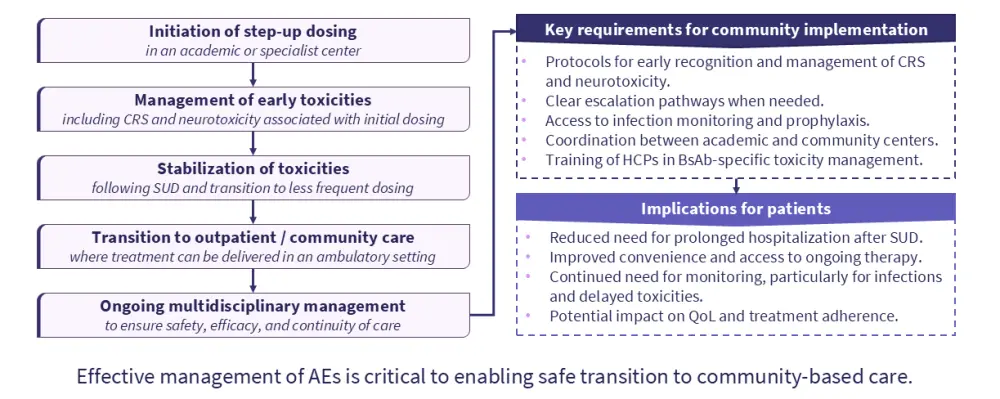
Figure 2. Management of BsAb-associated toxicities in the community*
Key points
- BCMA-directed BsAbs provide an off-the-shelf immunotherapy option for the treatment of MM, with broadly comparable efficacy and safety profiles across currently approved agents.3
- Selection of BCMA-directed BsAbs is influenced by multiple factors, including disease burden, treatment urgency, prior therapies, T-cell fitness, patient preferences, and access to treatment.3
- The International Myeloma Working Group (IWMG) consensus recommendations suggest, when feasible, CAR T-cell therapy is generally preferred for eligible patients; however, BCMA-directed BsAbs may be particularly valuable for patients requiring rapid treatment initiation or those unable to access CAR T-cell therapy.4
- Responses to subsequent BCMA-targeted therapies may be less frequent and less durable following prior BCMA-directed treatment, highlighting the importance of considered treatment sequencing.4
- Combination regimens and earlier-line use of BCMA-directed bispecific antibodies are being investigated with the aim of improving depth and durability of response, although long-term safety considerations remain important.5
- As BCMA-directed BsAbs move into earlier lines of therapy, further research is needed to better understand toxicity profiles, infection risk, and outcomes in different patient populations.5
- Step-up dosing and early monitoring are key components of treatment initiation, as cytokine release syndrome and neurotoxicity most commonly occur during the initial treatment period.1,2
- The transition of patients from specialist centers to community-based care has the potential to improve access and convenience but requires appropriate infrastructure, training, and multidisciplinary coordination.1,2
- Standardized protocols, clear escalation pathways, and patient education are essential to support early recognition and management of treatment-related toxicities in community settings.1
- Expanding access to BCMA-directed bispecific antibodies requires continued collaboration between specialist and community centers to ensure safe and effective delivery of care.1
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content


