All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit the International Myeloma Foundation or HealthTree for Multiple Myeloma.
The Multiple Myeloma Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the Multiple Myeloma Hub cannot guarantee the accuracy of translated content. The Multiple Myeloma Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The Multiple Myeloma Hub is an independent medical education platform, sponsored by Abbvie, Roche, Bristol Myers Squibb, Pfizer, GSK, Johnson & Johnson, Legend Biotech and Caribou Biosciences. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account to access:
Bookmark & personalize site content
Receive alerts for new content in your areas of interest
View multiple myeloma content recommended for you
Approaches to measuring frailty in MM: Comparison of IMWG FI and PRFP
Frailty tools are often used in the assessment of patients with multiple myeloma (MM) to identify those who are at the highest risk for treatment intolerance, toxicity, and early mortality. Patients determined as frail are less frequently prescribed intense or ‘aggressive’ treatments, including those with some of the highest rates of response and overall survival. It is therefore vital to accurately categorize patients by frailty to prevent over- or under-treatment that could result in poorer outcomes.
Here, we summarize a publication by Murugappan et al.1 comparing the patient-reported frailty phenotype (PRFP) and the International Myeloma Working Group Frailty Index (IMWG FI) approaches to measuring frailty.
Methods1
- In this comparison, the PRFP and IMWG FI were evaluated for their benefits, limitations, and concordance in classification of frailty in relapsed/refractory multiple myeloma (RRMM).
- Data were collated from six phase II randomized clinical trials in RRMM, in which 2,750 patients were classified as either fit, intermediate fit, or frail using both the PRFP and IMWG FI.
- A weighted Cohen’s kappa was utilized to establish concordance between the tools.
Key findings1
- Of the total population, 29.5% (n = 811) were identified as frail by at least one of the frameworks.
- Overall, a larger number of patients were classified as frail using the PRFP at 21.7% compared with 16.4% in the IMWG FI (Table 1).
- In general, there was fair agreement between the IMWG FI and PRFP using Cohen’s kappa, at 0.34 [0.31 – 0.37], with a categorization overlap of 29% (Figure 1).
Table 1. Classification of frailty by IMWG FI and PRFP tools*
|
IMWG FI, International Myeloma Working Group Frailty Index; PRFP, patient-reported frailty phenotype. |
||
|
Frailty status, % |
IMWG FI |
PRFP |
|---|---|---|
|
Frail |
16.4 |
21.7 |
|
Intermediate/pre-frail |
28.1 |
24.5 |
|
Fit |
55.5 |
53.8 |
Figure 1. Overlap in categorization of frailty by the IMWG FI and the PRFP*
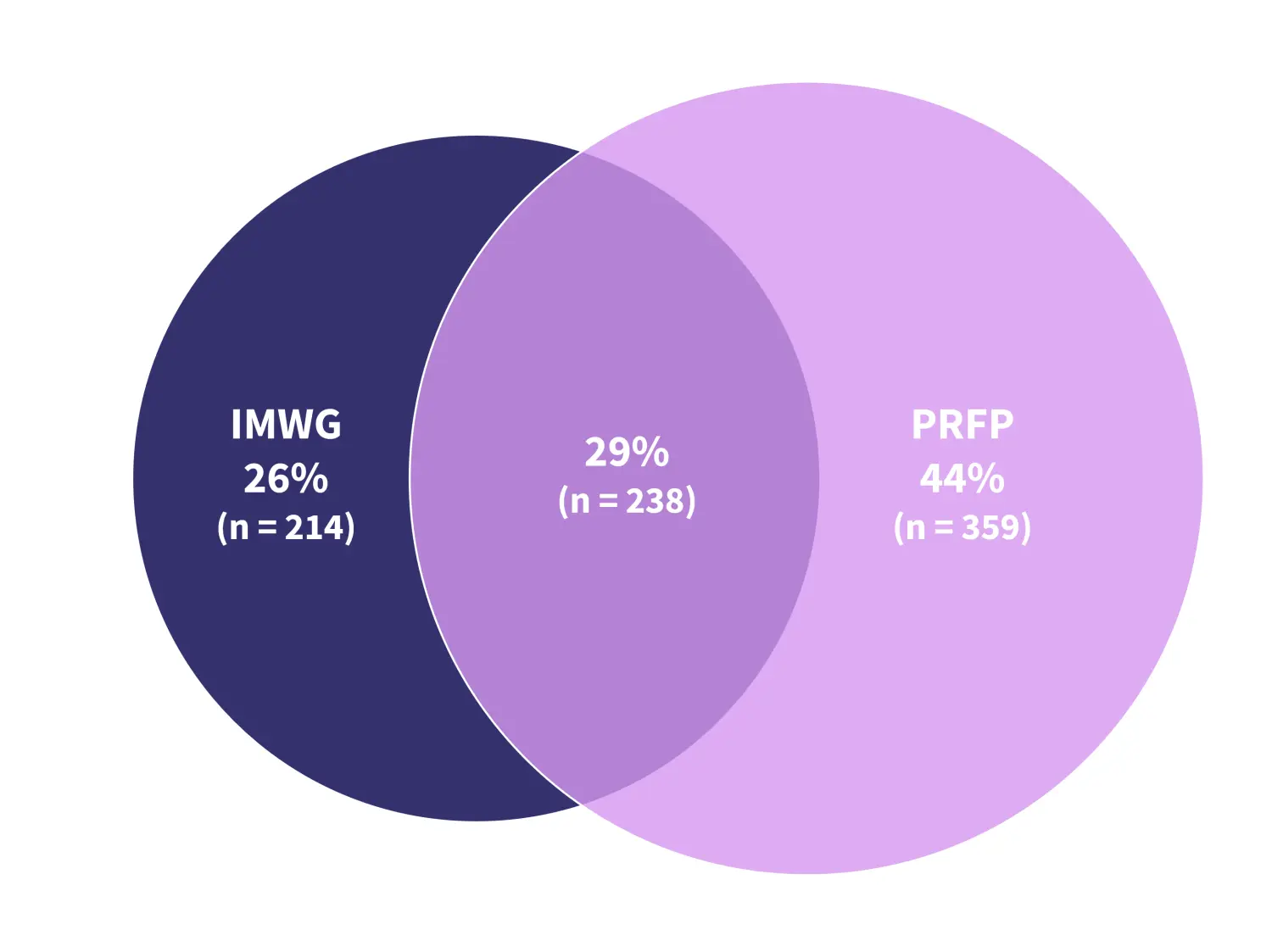
IMWG, International Myeloma Working Group; PRFP, patient-reported frailty phenotype.
*Adapted from Murugappan, et al.1
Framework limitations
- A limitation of the IMWG FI is the reliance on chronological age as a determinant of frailty.
- All patients aged >80 years are classified as frail, regardless of biological or functional status, which inhibits the ability to identify frailty in younger patients.
- IMWG FI is further limited by a reliance on activities of daily living as a measure of functional capacity.
- Activities of daily living may be biased by gender and culture, with questions referring to household activities, such as laundry and cooking, making them unrepresentative of daily life for some patients.
- A considerable limitation of the PRFP is the lack of validation in the newly diagnosed population, where the IMWG FI was initially developed.
|
Key learnings |
|---|
|
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content

