All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a healthcare professional. If you are a patient or carer, please visit the International Myeloma Foundation or HealthTree for Multiple Myeloma.
The Multiple Myeloma Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the Multiple Myeloma Hub cannot guarantee the accuracy of translated content. The Multiple Myeloma Hub and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


The Multiple Myeloma Hub is an independent medical education platform, sponsored by Abbvie, Roche, Bristol Myers Squibb, Pfizer, GSK, Johnson & Johnson, Legend Biotech and Caribou Biosciences. Funders are allowed no direct influence on our content. The levels of sponsorship listed are reflective of the amount of funding given. View funders.
Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account to access:
Bookmark & personalize site content
Receive alerts for new content in your areas of interest
View multiple myeloma content recommended for you
Treatment pathways and patient attrition across lines of therapy: The French experience
The distinct characteristic of multiple myeloma (MM) is its ability of relapsing-remitting in succession, consequently defining the lines of treatment in patients with MM. Despite remission after first-line treatment, many patients in due course relapse, and the duration of response decreases with subsequent therapies. Treatment becomes more challenging after each relapse as the disease augments resistance to multiple therapies. Additionally, following each relapse, the cumulative toxicity of therapies increases; therefore, exploring the treatment pathway in patients with MM is needed.
During the 18th International Myeloma Workshop (IMW 2021), Aurore Perrot presented a comprehensive overview of the evolution of treatment lines in patients with MM from their study ‘Multiple myeloma: An epidemiological study using SNIIRAM database’ or MYLORD.1 The Multiple Myeloma Hub is pleased to provide a summary of the presentation below.
Study design
This was a retrospective, observational cohort study using the French administrative health care database (SNIIRAM/SNDS) in patients treated for MM in France during 2014–2019. Patients with a treatment history were identified using an artificial intelligence algorithm (ATLAS) (Figure 1), and treatment lines were reconstructed for these patients to understand the evolution of therapeutic management of MM.
The primary objective was to describe treatment pathways and attrition rates across lines of treatments in patients with MM. The outcomes of interest included:
- Time to next treatment (TTNT)
- Overall survival (OS)
- Treatment sequencing
Figure 1. Patient selection process*
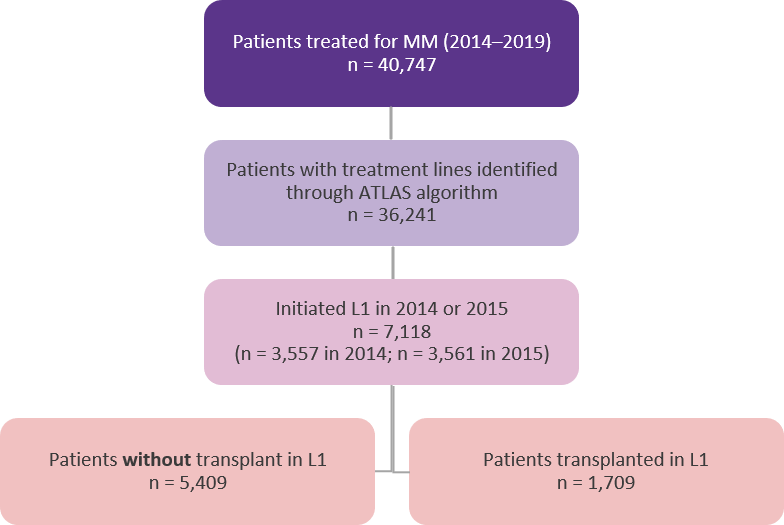
L1, first line of therapy; MM, multiple myeloma.
*Adapted from Perrot et al.1
Results
Baseline characteristics
A total of 7,118 patients were included in the study, the median age was 71 years (interquartile range [IQR], 62–79 years) and 51% of patients were male. The most common comorbidities included cardiovascular and neurovascular diseases (33%), diabetes (15%), concomitant solid tumor (10%), and renal failure (3%).
Outcomes
- The 5-year OS rate was 41% and 75% in patients who did not undergo transplantation and those who did, respectively. As expected, the cohort of patients without frontline transplant were older (median, 71 years old) than those eligible for transplant as first line of therapy (median, 60 years).
- Attrition rates were higher in the subgroup not transplanted in frontline, mainly due to a higher number of deaths in early lines of treatment (Figure 2).
Figure 2. Attrition rates of patients with transplant versus without transplant in first line of treatment (L1)*

L, line of therapy.
*Adapted from Perrot et al.1
- Patients with transplant in first line of therapy (L1) had a decreasing median TTNT of 40, 20, and 10 months after L1, second line of therapy (L2), and third line of therapy (L3), respectively.
- The median TTNT in patients who did not undergo a transplant in L1 was 29, 26, and 15 months for L1, L2, and L3, respectively. The median TTNT was similar between L1 and L2.
- The most common treatment sequences during 2014–2015 for L1 included bortezomib (V)-based regimens: bortezomib, melphalan, and prednisone (VMP) for patients without transplant in L1, and daratumumab plus bortezomib, thalidomide, and dexamethasone (Dara-VTd) for patients undergoing transplantation (Figure 3).
Figure 3. Most frequent treatment sequences used in 2014–2015*

Dara mono, daratumumab monotherapy; L1, first line of therapy; Pd, pomalidomide and dexamethasone; Rd, lenalidomide and dexamethasone; VMP, bortezomib, melphalan, and prednisone; VTd, bortezomib, thalidomide, and dexamethasone.
*Adapted from Perrot et al.1
Conclusion
This large-scale, retrospective cohort study demonstrated that real-world data can be used to compare treatment lines and their effectiveness providing a precise analysis of optimal treatment sequences in patients with MM, including their impact on the OS. Most patients with MM do not have the opportunity to be treated with several lines of treatment. However, this study demonstrated that new treatments should be initiated as early as possible in these patients. The MYLORD study is on-going, and further findings will be presented.
References
Please indicate your level of agreement with the following statements:
The content was clear and easy to understand
The content addressed the learning objectives
The content was relevant to my practice
I will change my clinical practice as a result of this content